Root cause analysis (RCA) is one of the most valuable problem-solving methods used throughout manufacturing, aerospace, defense, healthcare, construction, and countless other industries. When performed correctly, it helps organizations eliminate recurring problems rather than repeatedly correcting the same symptoms.
Many organizations respond to nonconformances by replacing damaged parts, retraining an employee, or issuing a corrective action without determining why the issue occurred. While these actions may temporarily resolve the immediate problem, they rarely prevent the problem from happening again.
Root cause analysis changes the focus from “What happened?” to “Why did it happen?”
Whether investigating customer complaints, production defects, failed inspections, warranty claims, equipment failures, or supplier quality issues, a structured root cause analysis helps identify the underlying process failure so corrective actions address the actual cause instead of the visible symptom.
What Is Root Cause Analysis?
Root cause analysis is a structured investigation used to identify the underlying cause of a problem. Rather than treating the immediate issue, the objective is to determine the process failure that allowed the problem to occur.
For example:
A customer receives a component with an incorrect hole diameter.
The immediate problem is the oversized hole.
However, the root cause may involve:
- Tool wear
- Incorrect CNC programming
- Missing inspection requirements
- Poor revision control
- Calibration issues
- Inadequate operator training
- Lack of process verification
Unless the true cause is identified and eliminated, the problem is likely to occur again.
Why Root Cause Analysis Matters
Every recurring quality problem consumes time, labor, materials, and customer confidence.
Organizations that consistently perform effective root cause analyses often experience:
- Reduced scrap
- Fewer customer complaints
- Lower rework costs
- Improved production efficiency
- Better supplier performance
- Stronger corrective action programs
- Improved audit results
- Increased customer confidence
Effective root cause analysis also supports continual improvement by identifying weaknesses in processes before they develop into larger quality issues.
Symptoms vs. Root Causes
One of the most common mistakes is confusing symptoms with root causes.
A symptom is the visible result of a problem.
A root cause explains why the problem occurred.
| Symptom | Possible Root Cause |
|---|---|
| Incorrect part shipped | Revision control failure |
| Wrong material received | Purchasing verification process ineffective |
| Missing weld | Inspection operation omitted |
| Failed dimensional inspection | Worn tooling not replaced |
| Customer complaint | Process controls inadequate |
| Missing documentation | Document control procedure ineffective |
| Repeated NCRs | Corrective actions ineffective |
| Calibration overdue | Asset management process failed |
Simply correcting the symptom rarely prevents recurrence.
Characteristics of an Effective Root Cause
An effective root cause should:
- Explain why the problem occurred.
- Be supported by objective evidence.
- Identify a process failure.
- Be capable of being corrected.
- Prevent recurrence when corrected.
Poor root cause statement:
Operator forgot to inspect the part.
Improved root cause statement:
The inspection plan did not require independent verification before shipment.
The difference is significant.
One blames a person.
The other identifies a process weakness.
Common Problems That Require Root Cause Analysis
Root cause analysis is commonly used to investigate:
- Customer complaints
- Product defects
- Supplier nonconformances
- Production delays
- Equipment failures
- Safety incidents
- Warranty claims
- Audit findings
- Process failures
- Documentation errors
- Calibration failures
- First Article Inspection discrepancies
Whenever a problem has the potential to recur, root cause analysis should be considered.
The Root Cause Analysis Process
Although organizations use different methodologies, most successful investigations follow a similar sequence.
1. Clearly Define the Problem
Begin by describing exactly what occurred.
Include objective information such as:
- What happened
- Where it occurred
- When it occurred
- Who identified it
- How many parts were affected
- Customer impact
Avoid assumptions.
Poor statement:
Parts are bad.
Better statement:
Three parts failed dimensional inspection because hole diameter exceeded the upper tolerance limit by 0.006 inch.
Specific problems produce better investigations.
2. Contain the Problem
Before determining the cause, prevent additional nonconforming products from reaching the customer.
Containment activities may include:
- Stopping production
- Segregating inventory
- Holding shipments
- Inspecting affected lots
- Notifying customers
- Reviewing previous production
Containment protects customers while the investigation continues.
3. Collect Objective Evidence
Evidence should support every conclusion.
Examples include:
- Engineering drawings
- Inspection reports
- Calibration records
- Process travelers
- Machine logs
- Training records
- Purchase orders
- Material certifications
- Operator interviews
- Photographs
Evidence should replace assumptions.
4. Identify Contributing Factors
Rarely does one issue exist alone.
Investigators should evaluate:
- Equipment
- Materials
- Environment
- Procedures
- Documentation
- Personnel
- Measurement methods
- Inspection frequency
These factors often reveal patterns leading toward the actual root cause.
5. Determine the Root Cause
Use structured analysis rather than guessing.
Ask:
- Why did this occur?
- Why was the process unable to prevent it?
- Why was it not detected earlier?
- Why did existing controls fail?
Continue until the investigation identifies the underlying process failure.
6. Implement Corrective Actions
Corrective actions should eliminate the root cause.
Examples include:
- Updating procedures
- Revising inspection plans
- Implementing tooling replacement schedules
- Adding verification checkpoints
- Revising work instructions
- Improving document control
- Updating training requirements
Simply replacing the defective part is correction—not corrective action.
7. Verify Effectiveness
Verification confirms the corrective action actually solved the problem.
Organizations may verify effectiveness through:
- Follow-up inspections
- Internal audits
- Customer feedback
- Process monitoring
- Statistical data
- Reduced NCR trends
Without verification, there is no evidence the corrective action worked.
Root Cause Analysis Tools
Several proven techniques are available to identify root causes. The most effective tool depends on the complexity of the problem, the available evidence, and the organization’s processes. In many investigations, multiple tools are used together rather than relying on a single method.
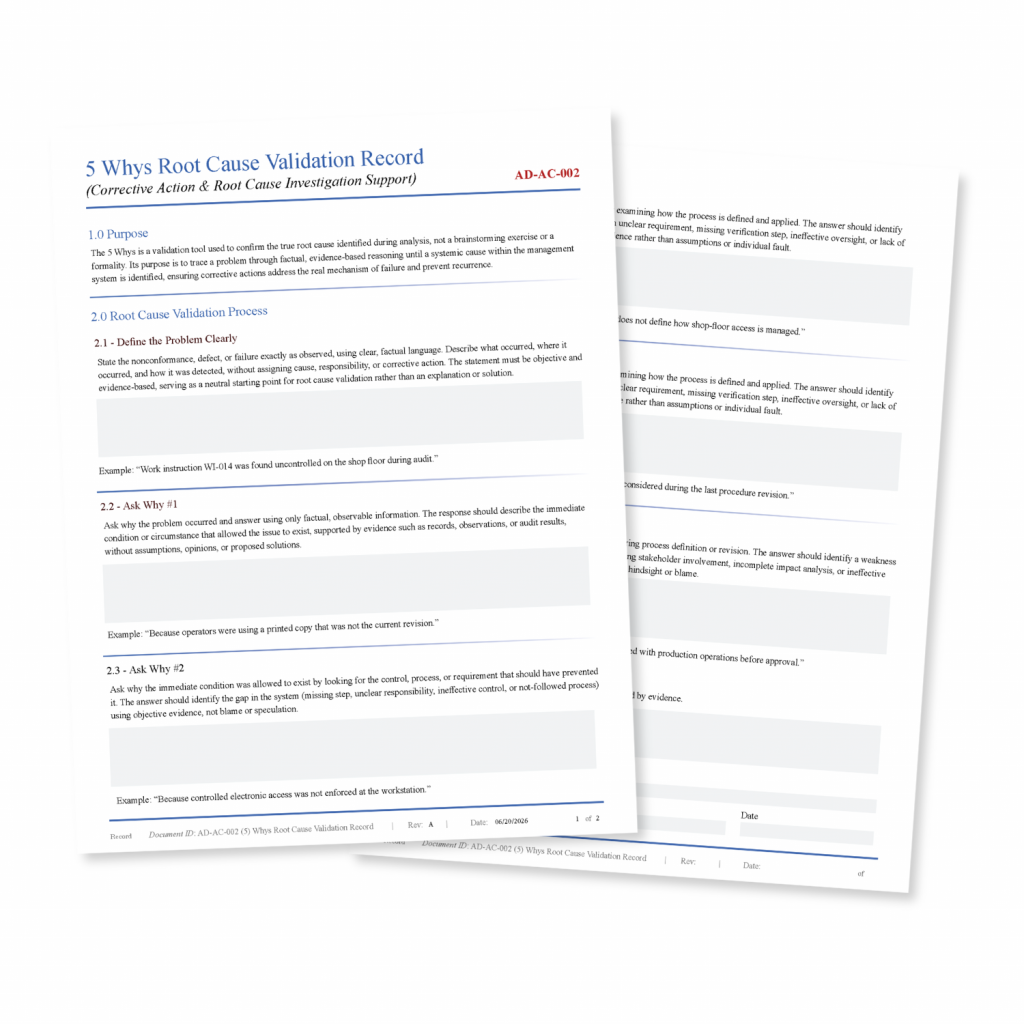
The 5 Whys
The 5 Whys method is one of the simplest and most widely used root cause analysis techniques. Rather than stopping at the first explanation, investigators repeatedly ask “Why?” until the underlying process failure is identified.
The goal is not to ask exactly five questions. Some investigations require three questions, while others require seven or more. The important objective is to continue questioning until additional “why” questions no longer reveal a deeper process issue.
Example
Problem:
A customer received a component with an oversized hole.
Why?
The hole was machined too large.
Why?
The cutting tool exceeded its wear limit.
Why?
The tool was not replaced.
Why?
There was no scheduled tool life replacement program.
Why?
Preventive maintenance requirements were never established during process planning.
Notice how the investigation moved beyond blaming the machinist. The true root cause was inadequate process planning.
Fishbone Diagram (Cause and Effect Diagram)
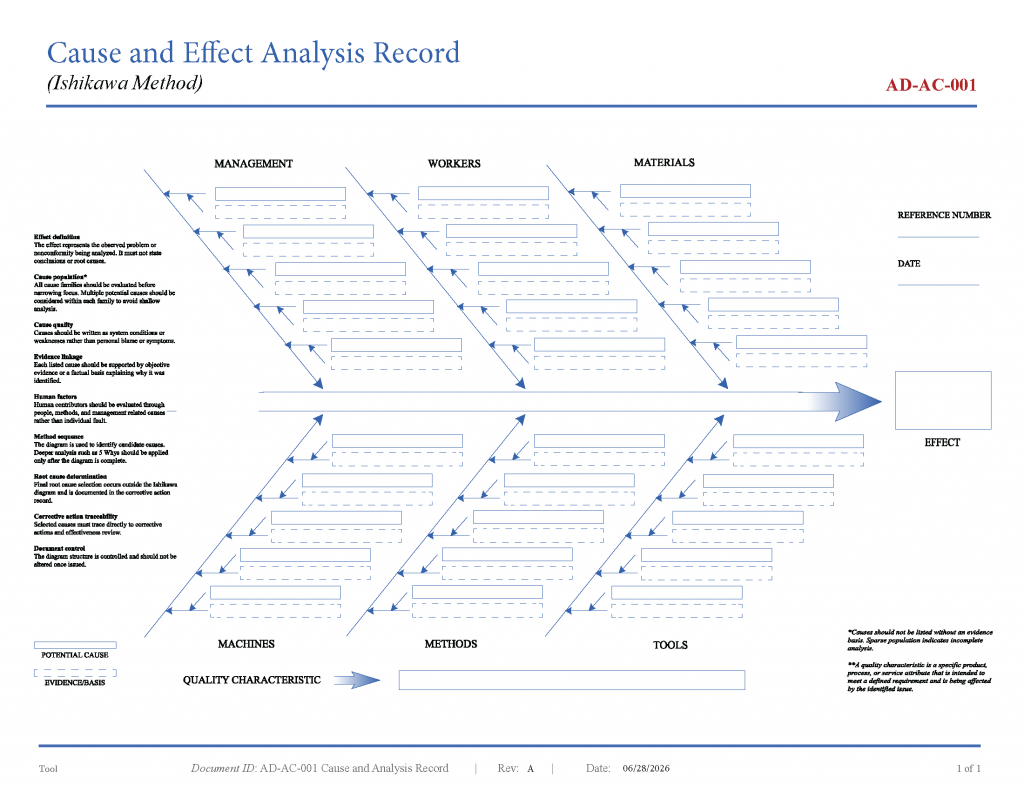
A Fishbone Diagram, sometimes called an Ishikawa Diagram, organizes potential causes into logical categories.
One of the most common versions used in manufacturing includes the Six Ms:
- Man (People)
- Machine
- Method
- Material
- Measurement
- Mother Nature (Environment)
Each category is examined for possible contributors to the problem.
For example, if a machined feature fails inspection:
People
- Training inadequate
- Operator fatigue
- Incorrect setup
Machine
- Worn spindle
- Improper calibration
- Tool chatter
Method
- Incorrect work instruction
- Missing inspection point
- Poor setup procedure
Material
- Incorrect alloy
- Material hardness variation
- Supplier defect
Measurement
- Calibration expired
- Wrong inspection equipment
- Measurement technique inconsistent
Environment
- Temperature variation
- Poor lighting
- Contamination
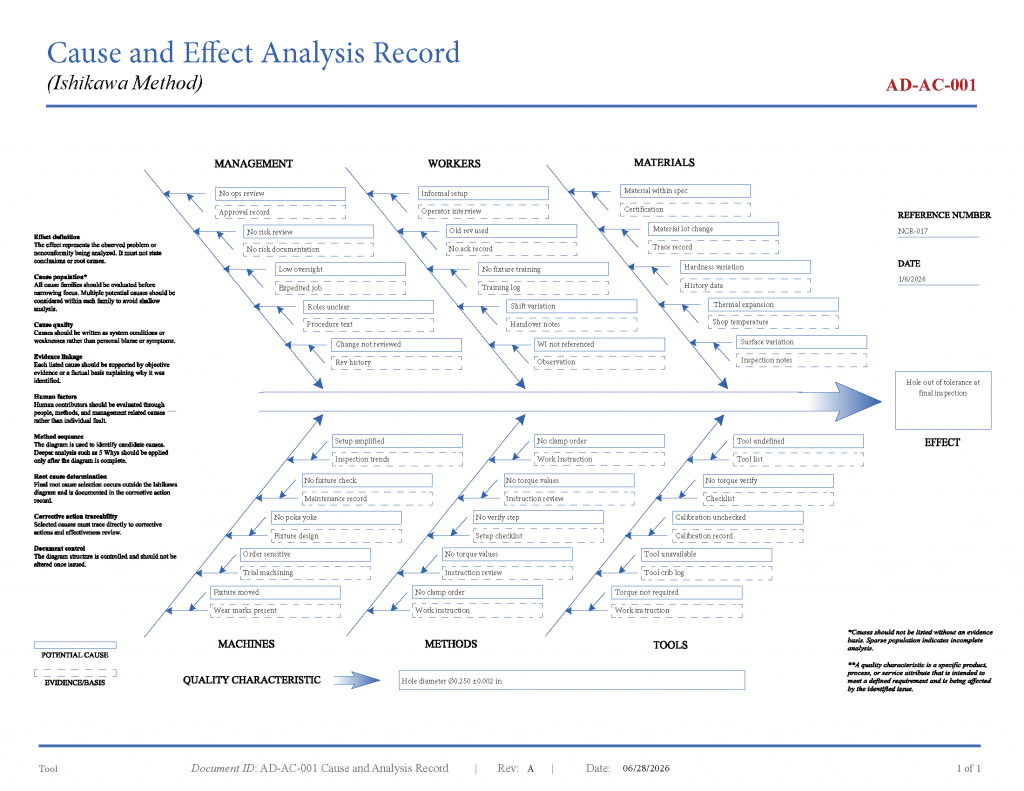
The Fishbone Diagram is particularly effective during team investigations because it encourages discussion while ensuring no major category is overlooked.
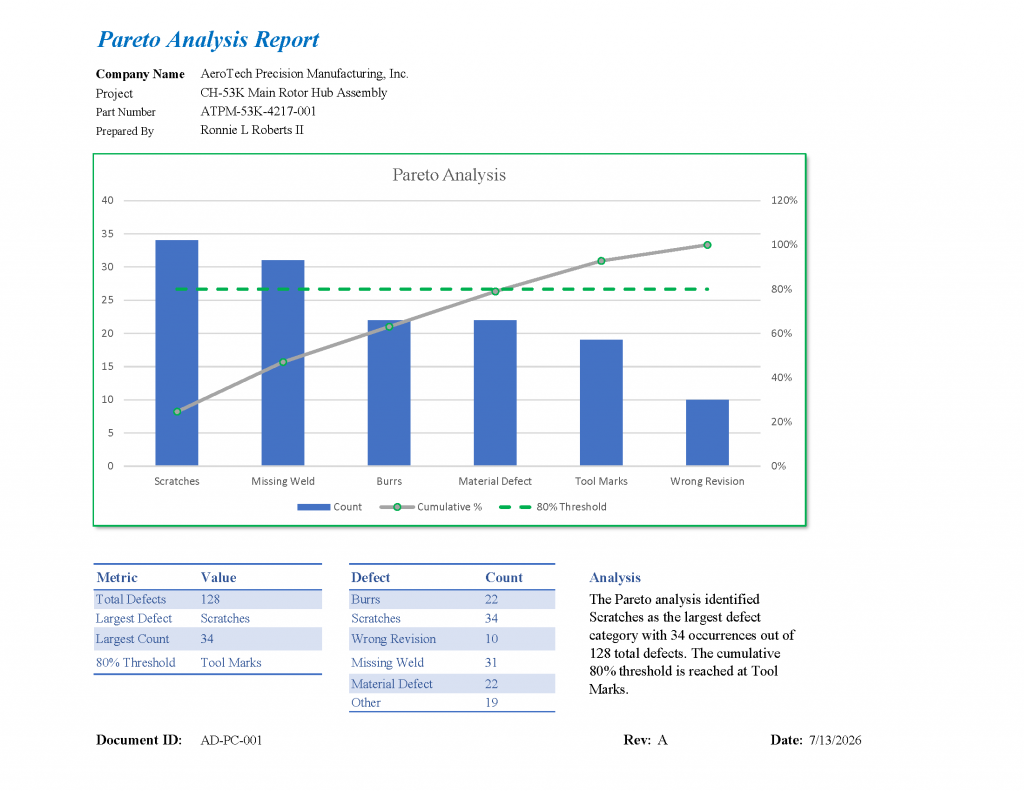
Pareto Analysis
Pareto Analysis prioritizes problems by identifying the relatively small number of causes responsible for most quality issues.
For example:
| Defect | Quantity |
|---|---|
| Burrs | 96 |
| Missing documentation | 42 |
| Scratches | 31 |
| Wrong revision | 18 |
| Missing hardware | 12 |
Instead of addressing every issue equally, resources are focused on the largest contributors.
Organizations frequently discover that a handful of recurring defects account for most nonconforming products.
Process Mapping
Many quality problems occur because the actual process differs from the documented process.
Creating a process map helps investigators visualize:
- Inputs
- Process steps
- Decision points
- Inspection operations
- Outputs
When compared to actual production activities, missing controls often become obvious.
Examples include:
- Missing inspection operations
- Uncontrolled document revisions
- Incomplete approvals
- Undefined responsibilities
Process mapping is especially valuable when investigating documentation and workflow failures.
Failure Mode and Effects Analysis (FMEA)
Unlike other root cause analysis tools, FMEA is proactive.
Rather than investigating a failure that already occurred, FMEA attempts to identify potential failures before production begins.
Organizations evaluate:
- Potential failure modes
- Causes
- Effects
- Existing controls
- Risk priority
Although FMEA is primarily a preventive tool, previous FMEA documentation can provide valuable information during root cause investigations.
Selecting the Right Tool
No single technique works for every investigation.
| Situation | Recommended Tool |
|---|---|
| Simple recurring issue | 5 Whys |
| Multiple possible causes | Fishbone Diagram |
| Trend analysis | Pareto Chart |
| Workflow problems | Process Mapping |
| High-risk product development | FMEA |
| Complex investigations | Combination of tools |
Experienced investigators often combine several methods to build objective evidence before determining the final root cause.
Manufacturing Example: Step-by-Step Root Cause Analysis
A defense contractor receives a customer complaint after a dimensional inspection identifies an oversized hole during receiving inspection.
Problem Statement
Hole diameter:
Specified nominal dimension: 0.500 ±0.002
Measured:
0.505 inch
Ten components were shipped.
Three exceeded tolerance.
Immediate Containment
Quality immediately:
- Stops production.
- Places remaining inventory on hold.
- Identifies all affected lots.
- Notifies the customer.
- Begins 100% inspection of completed inventory.
Containment prevents additional nonconforming products from reaching the customer.
Collect Evidence
The investigation gathers:
- Engineering drawing
- CNC program
- Inspection reports
- Calibration certificates
- Tool offset history
- Tool replacement records
- Operator training records
- Traveler
- Process planning documentation
Each document provides objective evidence supporting the investigation.
Initial Findings
Inspection equipment was calibrated.
Drawing revision was correct.
Operator followed documented instructions.
Material certification acceptable.
No programming errors identified.
Attention shifts toward machining operations.
5 Whys Investigation
Why was the hole oversized?
The cutting tool produced an oversized feature.
Why did the tool produce oversized holes?
The tool exceeded acceptable wear.
Why wasn’t the tool replaced?
No replacement interval existed.
Why was no interval established?
The machining process never defined expected tool life.
Why was tool life never established?
Process planning focused on production efficiency without developing preventive controls.
Root Cause
No documented tool life management process existed.
Corrective Actions
Instead of disciplining the machinist, the organization:
- Establishes documented tool life limits.
- Adds replacement intervals.
- Updates work instructions.
- Revises inspection frequency.
- Requires first-piece verification after tool replacement.
- Trains operators.
- Updates process planning documentation.
The process improves rather than simply replacing defective parts.
Verification of Effectiveness
Three months later:
- No oversized holes reported.
- Internal audit confirms compliance.
- Customer complaints reduced.
- Inspection data demonstrates process stability.
The corrective action is considered effective because objective evidence confirms the issue has not recurred.
This example demonstrates an important principle of root cause analysis: effective investigations improve the process rather than assigning blame. When organizations focus on systemic weaknesses instead of individual mistakes, corrective actions are more likely to produce lasting improvements.
Common Root Cause Analysis Mistakes
Many organizations conduct root cause analyses after nonconformances, customer complaints, or audit findings. However, simply completing an investigation does not mean the true cause has been identified. The following mistakes frequently result in recurring problems and ineffective corrective actions.
Stopping the Investigation Too Early
One of the most common errors is accepting the first explanation without investigating further.
Example:
Problem: Hole diameter exceeds tolerance.
Incorrect conclusion:
The operator drilled the hole incorrectly.
This statement describes what happened but not why it happened.
A more thorough investigation may reveal:
- Worn cutting tools
- Missing inspection frequencies
- Incorrect setup documentation
- Outdated work instructions
- Missing process controls
The deeper investigation identifies a process failure rather than assigning blame.
Blaming People Instead of Processes
People make mistakes, but quality systems should be designed to prevent or detect those mistakes before they reach the customer.
Poor root cause:
Employee failed to inspect the part.
Improved root cause:
The inspection plan did not require verification of the critical characteristic before shipment.
The first conclusion focuses on an individual.
The second identifies a weakness in the quality management system.
Confusing Corrections with Corrective Actions
These terms are often used interchangeably, but they serve different purposes.
A correction addresses the immediate problem.
A corrective action eliminates the cause of the problem.
| Correction | Corrective Action |
|---|---|
| Replace defective part | Revise machining process |
| Rework product | Update inspection frequency |
| Replace damaged component | Implement preventive maintenance |
| Retrain operator | Revise work instructions and process controls |
Replacing a defective part may satisfy today’s shipment, but it does nothing to prevent tomorrow’s defect.
Failing to Collect Objective Evidence
Quality investigations should be supported by evidence rather than assumptions.
Useful evidence includes:
- Inspection reports
- Calibration certificates
- Engineering drawings
- Machine logs
- Training records
- Purchase orders
- Material certifications
- Photographs
- Customer complaints
- Production travelers
Every conclusion should be traceable to objective information.
Ignoring Contributing Factors
Many quality problems involve multiple contributing factors.
Example:
A defective assembly may involve:
- Poor documentation
- Worn tooling
- Supplier material variation
- Inadequate inspection
- Incorrect work instructions
Focusing on only one factor may leave other process weaknesses uncorrected.
Failing to Verify Effectiveness
Corrective actions should never be considered complete immediately after implementation.
Organizations should verify effectiveness using measurable evidence.
Examples include:
- Reduced defect rates
- Improved process capability
- Follow-up audits
- Customer feedback
- Inspection data
- Statistical process monitoring
Without verification, there is no objective evidence that the corrective action solved the problem.
Root Cause Analysis Best Practices
Organizations that consistently perform effective investigations often follow several common practices.
Define the Problem Clearly
Avoid vague descriptions.
Poor:
Parts failed inspection.
Better:
Five machined components exceeded the upper diameter tolerance by 0.004 inch during final inspection.
Specific problem statements produce focused investigations.
Build a Cross-Functional Team
Complex investigations often benefit from multiple perspectives.
Potential participants include:
- Quality personnel
- Manufacturing engineers
- Production supervisors
- Machine operators
- Maintenance technicians
- Purchasing representatives
- Supplier quality engineers
Different departments often identify causes others may overlook.
Focus on Facts
Investigations should rely on measurable information.
Avoid statements beginning with:
- I think…
- Probably…
- It seems…
- Maybe…
Instead use:
- Inspection records
- Measurement data
- Production history
- Document revisions
- Audit results
Facts produce stronger corrective actions.
Document Every Step
Good documentation supports:
- Customer confidence
- Internal audits
- Regulatory compliance
- Organizational learning
- Future investigations
Well-documented investigations also make recurring trends easier to identify.
Frequently Asked Questions
What is the purpose of root cause analysis?
Root cause analysis identifies the underlying process failure responsible for a problem so corrective actions eliminate the cause rather than repeatedly addressing the symptoms.
How many “Why” questions should be asked?
There is no required number.
Continue asking until additional questions no longer identify a deeper process failure.
Sometimes three questions are sufficient.
Other investigations require considerably more.
Can a problem have multiple root causes?
Yes.
Complex manufacturing problems often result from multiple independent failures occurring simultaneously.
Examples include:
- Poor documentation
- Inadequate training
- Missing inspections
- Equipment wear
- Supplier variation
Each contributing process should be evaluated independently.
Who should perform root cause analysis?
The investigation should involve personnel familiar with the affected process.
Depending on the issue, this may include:
- Quality Engineers
- Quality Inspectors
- Manufacturing Engineers
- Production Supervisors
- Operators
- Maintenance personnel
- Supplier Quality Engineers
Cross-functional participation often improves investigation quality.
When should root cause analysis be performed?
Root cause analysis is commonly initiated following:
- Customer complaints
- Product defects
- Internal audit findings
- Supplier nonconformances
- Safety incidents
- Equipment failures
- Warranty claims
- Repeated production issues
- Corrective action requests
Is root cause analysis required by AS9100?
AS9100 requires organizations to address nonconformities by determining their causes, implementing corrective actions, and verifying effectiveness. While the standard does not mandate a specific root cause analysis method, organizations must demonstrate that corrective actions address the underlying cause of the nonconformity rather than only the immediate issue.
Downloadable Root Cause Analysis Resources
A structured investigation becomes significantly easier when consistent documentation is used.
Useful resources include:
- Root Cause Analysis Checklist
- 5 Whys Worksheet
- Fishbone Diagram Template
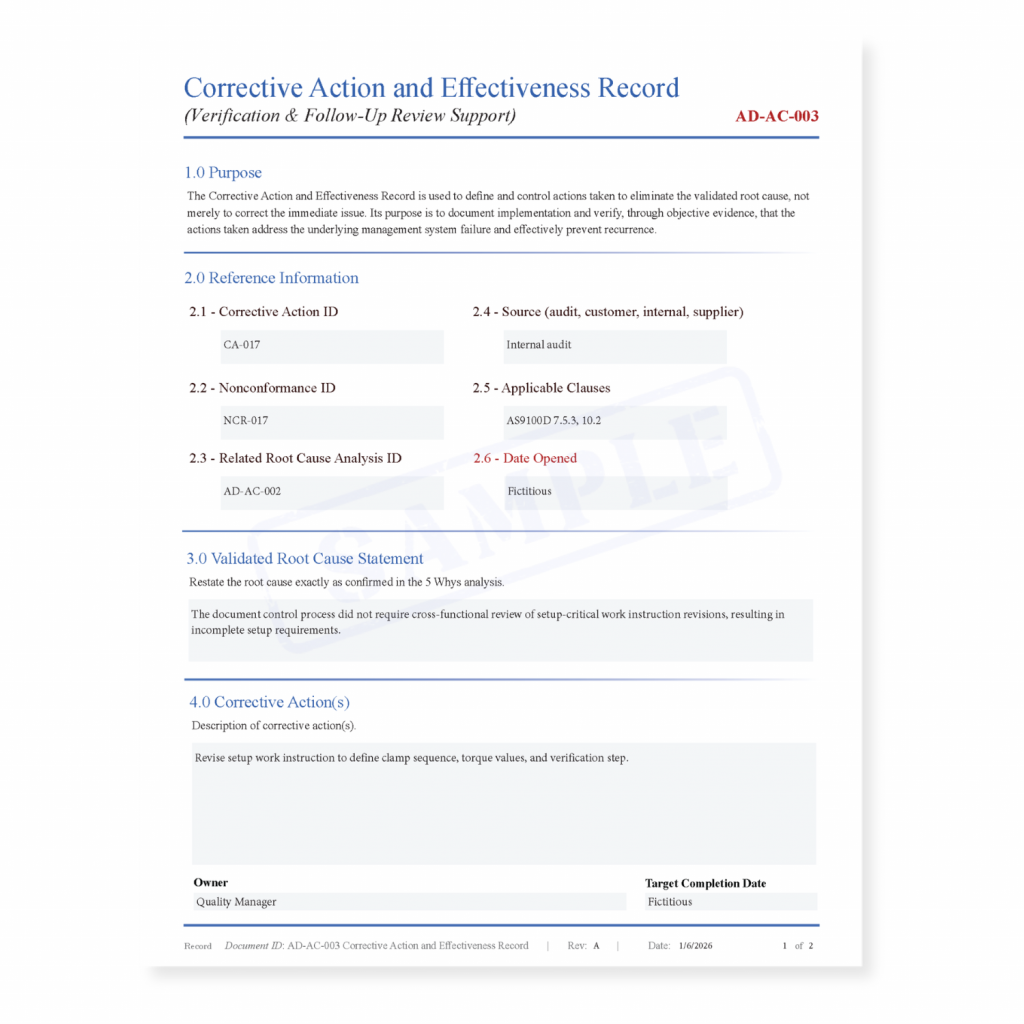
- Corrective Action Form
- Investigation Planning Worksheet
- Objective Evidence Checklist
- Corrective Action Verification Form
Using standardized forms helps ensure investigations remain consistent, complete, and supported by objective evidence.
Conclusion
Root cause analysis is more than a quality tool. It is a disciplined approach to understanding why problems occur and how to prevent them from happening again.
Organizations that focus only on correcting defects often experience the same issues repeatedly. Those that investigate process failures, collect objective evidence, implement meaningful corrective actions, and verify effectiveness build stronger quality systems, reduce costs, improve customer satisfaction, and support continual improvement.
Whether investigating a customer complaint, production defect, supplier issue, or audit finding, effective root cause analysis should always seek to improve the process rather than assign blame. When organizations eliminate the underlying causes of nonconformities, they create more reliable processes, more consistent products, and stronger long-term operational performance.